The indication for a joint replacement of the shoulder, hip or knee must always be based on a comprehensive medical history, a clinical examination and appropriate radiological diagnostics. The correct indication is decisive for the success of the therapy for each individual patient.
During the clinical examination, the joint mobility of the affected joint is assessed in a side comparison, structures close to the joint such as muscles and tendons are tested for functionality and special pain and stability tests are applied. The radiological diagnostics must take into account the particularity of the joint in each case and includes X-rays, special X-ray stress images supplemented by magnetic resonance imaging and, if necessary, computer tomography. On the basis of these imaging diagnostics, the joint specialist sees the typical signs of osteoarthritis such as joint space narrowing, joint deformities and marginal attachments. Only when these objectifiable criteria are available and match the patient's personal level of suffering is the basis for the decision to replace the affected joint completely or partially.

Severe arthrosis using the example of the hip joint
The shoulder is a very important joint, especially for the overhead athlete. The large radius of movement that our hand needs for optimal use is ensured by the design of the arm as a link chain and the special mobility of the shoulder joint and shoulder girdle.
The special feature of the ball joint shoulder is that the glenoid cavity is small compared to the ball, the humeral head. Think of it like comparing golf tee to golf ball. Because the glenoid cavity is small, stabilisation at the shoulder joint requires the strength of a well-trained musculature, the so-called rotator cuff, which is why the shoulder is also referred to as a "friction-locked" joint.
The rotator cuff cannot be palpated because it is located deep below the shoulder cap muscle (deltoid muscle). The muscles of the rotator cuff move from the shoulder blade to the head of the humerus, where they attach their tendons and stabilise the head of the humerus in the small socket at the shoulder joint, which is an essential component of pain-free mobility of the upper arm in the shoulder joint. This applies to the natural shoulder as well as to the artificial joint.
In recent years, artificial joint replacement of the shoulder has become increasingly important. Good long-term results of established implant systems have strengthened the confidence in the known shoulder prostheses, which is confirmed by the constantly increasing number of operations. A decisive factor for the success of a shoulder endoprosthesis operation is that the surgeon selects the right prosthesis model for the respective shoulder disease. If an anatomical total shoulder endoprosthesis is fitted in the case of shoulder arthrosis, the rotator cuff mentioned above must be functionally intact, otherwise premature loosening will occur.

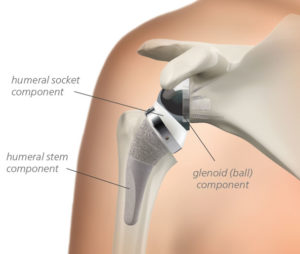
Anatomical, shaft-free shoulder prosthesis
In young patients with necrosis of the humeral head and a regular socket, only a replacement of the diseased humeral head can be made, a so-called hemiprosthesis.
The situation is different in the clinical picture of defective arthropathy, where a destroyed, non-reconstructable rotator cuff is the main problem. In this case, a normal anatomical shoulder prosthesis must not be fitted, as this would lead to premature loosening. Fortunately, today we have the inverse shoulder prosthesis as a successful therapy method.
Inverse shoulder prosthesis
Current movement analysis studies have shown that endoprosthetic replacement of the shoulder leads to a significant improvement in the maximum range of movement when performing everyday movements, which, along with pain reduction, is the decisive parameter for patient satisfaction.
Minimally invasive approaches to the hip joint have become more and more popular in recent years due to the increasing demand of patients to have the shortest possible hospital stay and quick rehabilitation. While 20 years ago, you as a patient still had inpatient stays of 2 weeks after a hip joint replacement with a classic approach, this has recently been reduced to a few days.
In order to enable short hospital stays, classical surgical techniques, which often required muscle detachment, were abandoned and replaced by minimally invasive approaches. These approaches respect the course of the musculature and tendon attachments and aim to minimise damage to muscles close to the joint. The AMIS approach is the anterior minimally invasive approach in which a natural muscle gap to the hip joint is used in a very elegant way. Muscles, tendons, vessels and nerves are pushed to the side.

So it is not the small skin incision that is crucial in AMIS access because it is not the skin that can make life difficult for patients after hip replacement surgery. It is the severed or injured muscles and tendons of the large muscles surrounding the hip joint that, once they are severed or injured, heal slowly and severely, sometimes not at all. The clear advantage of minimally invasive approaches is therefore that muscles, tendons and mechanoreceptors are preserved. The mechanoreceptors are important for our depth sensitivity and thus for a stable gait pattern. If we leave these structures intact during prosthesis implantation, the patient can start rehabilitation earlier after the procedure, the hospital stay is shortened and the patient returns more quickly to his or her individual daily activities such as golf.
In addition to the correct surgical method, the material and thus the durability of the respective prosthesis is decisive for a good long-term result. Here it is important to remember that modern hip prostheses are assembled from individual parts according to the modular principle: Acetabular cup, cup insert (inlay), ball head and hip stem.

Components of a hip endoprosthesis
During the operation, the modified femoral head including part of the neck of the femur is removed and then, after the modified acetabulum has been milled, an artificial cup is inserted into the pelvis and a prosthesis stem into the femur. Modern prostheses are made of different metal alloys (titanium, cobalt-chrome).
If the bone quality is good, cementless short shaft prostheses made of titanium alloys are often used nowadays. These are easy to implant minimally invasively and initially jam in the bone, which we call primary stability. Since the titanium surface is porous, the bone grows within a few months and fixes the prosthesis additionally, which is called secondary stability. In older patients with softer bone, e.g. due to osteoporosis, the cemented prosthesis is a very good solution.
The inlay is inserted into the socket as a running surface and the prosthesis head is attached to the prosthesis shaft. The movement then takes place between these two prosthesis parts, which we call sliding pairing. In the past, metal heads and polyethylene inlays were often used as sliding pairings. Due to the high abrasion of the polyethylene inlays at that time, however, strong abrasion-induced foreign body reactions occurred in many cases, which led to local bone dissolution with subsequent prosthesis loosening and resulted in alternating operations. The same problem occurred with hip cap prostheses, where a metal-metal sliding pairing was used. Metal-metal sliding pairings should no longer be used today due to the massive metal abrasion.
Instead, we now prefer modern ceramic-polyethylene and ceramic-ceramic sliding combinations, which have to meet ever higher demands due to the increased level of activity of our young patients. Therefore, the material properties of these pairings have been further improved in order to have the lowest possible abrasion of the pairing surfaces, which led to the development of modern ceramics and modern ultra-high cross-linked polyethylene with vitamin E. Today we have ideal conditions and a durability of more than 25 years is normal nowadays.
Nowadays, patients can also count on excellent durability for knee prostheses. Eight out of ten total knee endoprostheses today last for 25 years. If we compare the satisfaction of hip and knee prosthesis patients, 90% of patients are satisfied with the results after a hip joint replacement, compared to only 80% for the knee. In order to improve this value, a lot of research has been and is being done on the optimal implantation technique.

Total knee endoprosthesis
The challenge in knee joint replacement is that it is not a ball and socket joint like the hip, but rather the largest joint in the human body consisting of three partial joints, and these partial joints form a functional unit. The three partial joints must be taken into account when choosing the right joint replacement. Only then can an optimal result be achieved and the patient will ideally get a "forgotten knee" in addition to pain reduction and improved function, which means that he can use his new artificial knee joint in everyday life like the natural knee joint and forget that it is an artificial joint. The cause analysis of dissatisfied patients has shown that surgical factors such as implant alignment play a central role. If the artificial knee joint is installed with a rotation error, it cannot function, the patient suffers pain and has poor function.
This is where we discuss today which surgical technique is the best to install the artificial joint as precisely as possible. Until now, neither navigation nor patient-specific instruments have been able to show a significant superiority over conventional surgical techniques. Perhaps newer approaches such as kinematic alignment, which involves positioning the prosthesis strictly along the axes of rotation of the natural knee, will bring further improvement.
However, there is one important factor that we must not forget despite all the discussion about the progress of op techniques: The experienced surgeon who knows his trade and who reconstructs the knee joint kinematics optimally in three dimensions when fitting the knee joint is the decisive factor for success. Manual errors during prosthesis installation must be avoided at all costs - an experienced surgeon is more valuable - every new, seemingly groundbreaking surgical technique.
The design and materials of knee prostheses have been continuously improved in recent years, so that today, individual adaptation to the patient with maximum preservation of the non-damaged parts of the joint has become possible. The materials are now so good that they can last well over 20 years if correctly fitted.
In the past, the material was often suspected when patients had problems with their knee prosthesis. Today we know that it is not so much the material that fails but rather the surgeon. Studies show that manual errors such as rotation errors lead to poor results, especially in the knee joint.
The successful operation begins outside the operating room with an exact op planning including axis alignment, angle measurement, determination of the type of prosthesis and determination of the prosthesis size.
When selecting a prosthesis, the aim is to preserve as much of the body's own tissue structure as possible using the smallest possible implant (partial preservation). Corresponding to the three partial joints of the knee joint, each part can nowadays be replaced separately, which makes sense if the disease is limited to this part of the joint only. This means that there is a partial endoprosthesis on the inside or outside (sled prosthesis) and the joint surface behind the kneecap can also be replaced in isolation.
The most common partial joint replacement is the inner sled prosthesis for bowleg arthrosis of the knee. In this case, the inner side of the knee joint is replaced with a prosthesis and the remaining joint including cruciate ligaments is retained. With the correct indication and a clean surgical technique, excellent long-term results and a high level of patient satisfaction can be expected. Compared to full prostheses on the knee, partial prostheses are characterized by higher patient satisfaction, better mobility, lower surgical risks and a higher rate of "forgotten knees".

Inner sled prosthesis